I’ve been dealing with Cushing’s since 1983. The after effects of pituitary surgery since 1987, kidney cancer since 2006. It’s time I felt better, already!
From 1999 to today, not-so-quick recap from my bio:
1999 ~ Many people are now finding that they need HgH after pituitary surgery, so an Insulin Tolerance Test was performed. My endocrinologist painted a very rosey picture of how wonderful I’d feel on Growth Hormone. It sounded like a miracle drug to me!
I was only asked to fast before the ITT and to bring someone with me to take me home. There is no way I could have driven home. I got very cold during the test and they let me have a blanket. Also, though, lying still on that table for so long, my back hurt later. I’d definitely take – or ask for – a pillow for my back next time. They gave me a rolled up blanket for under my knees, too.
I don’t remember much about the test at all. I remember lying very still on the table. The phlebotomist took blood first, then tried to insert the IV (it took a few tries, of course). Then the endo himself put the insulin in through the IV and took the blood out of that. I remember the nurse kept asking me stupid questions – I’m sure to see how I was doing on the consciousness level. I’d imagine I sounded like a raving lunatic, although I believed that I was giving rational answers at the time.
Then everything just got black…I have no idea for how long, and the next thing I knew I was becoming aware of my surroundings again and the doctor was mumbling something. They gave me some juice and had me sit up very slowly, then sit on the edge of the table for a while. When I thought I could get up, they gave me some glucose tablets “for the road” and called my friend in. I was still kind of woozy, but they let her take me out, very wobbly, kind of drunk feeling.
My friend took me to a close-by restaurant – I was famished – but I still had trouble with walking and felt kind of dazed for a while. When I got home, I fell asleep on the sofa for the rest of the day.
But the most amazing thing happened. Saturday and Sunday I felt better than I had for 20 years. I had all this energy and I was flying high! It was so wonderful and I hoped that that was from the HgH they gave me to wake me up.
2001 ~ I had the ITT this morning. I don’t get any results until a week from Thursday, but I do know that I didn’t recover from the insulin injection as quickly as I did last time. The endo made a graph for my husband of me today and a “normal” person, although I can’t imagine what normal person would do this awful test! A normal person’s blood sugar would drop very quickly then rise again at about a right angle on the graph.
I dropped a little more slowly, then stayed very low for a long time, then slowly started to rise. On the graph, mine never recovered as much as the normal person, but I’m sure that I did, eventually.
The test this time wasn’t as difficult as I remember it being, which is good. Last time around, I felt very sweaty, heart pounding. I don’t remember any of that this time around. I do know that I “lost” about an hour, though. The phlebotomist took the first blood at 9:15, then the endo injected the insulin and took blood every 15 minutes after that. I counted (or remembered) only 4 of the blood draws, but it was 11:30 when they told me that my sugar wasn’t coming up enough yet and I’d have to stay another 30 minutes. It actually ended up being another hour.
Kim, the phlebotomist, asked me if I got a headache when they “crashed me” and I have no recollection of any of that.
Like last time, I was very, very cold, even with the blanket and my left arm – where the heplock was – fell asleep. Other than that – and my back hurting from lying on one of those tables all that time this wasn’t as bad as I remembered.
So, I waited for 10 days…
September 2004 ~ My new doctor was wonderful. Understanding, knowledgeable. He never once said that I was “too fat” or “depressed” or that all this was my own fault. I feel so validated, finally.
He looked through my records, especially at my 2 previous Insulin Tolerance Tests. From those, he determined that my growth hormone has been low since at least August 2001 and I’ve been adrenal insufficient since at least Fall, 1999 – possibly as much as 10 years! I was amazed to hear all this, and astounded that my former endo not only didn’t tell me any of this, he did nothing. He had known both of these things – they were in the past records that I took with me. Perhaps that was why he had been so reluctant to share copies of those records. He had given me Cortef in the fall of 1999 to take just in case I had “stress” and that was it.
The new endo took a lot of blood (no urine!) for cortisol and thyroid stuff. I’m going back on Sept. 28, 2004 for arginine, cortrosyn and IGF testing.
He has said that I will end up on daily cortisone – a “sprinkling” – and some form of GH, based on the testing the 28th.
October 2004 ~ I had cortrosyn and arginine-GHRH stimulation test at Johns Hopkins. They confirmed what the doctor learned from reading my 4 year old records – that I’m both adrenal-deficient and growth hormone-deficient. I started on my “sprinkle” (5 mg twice a day) of Cortef now and my new doctor has started the paperwork for GH so maybe I’m on my way…
November 2004 ~ Although I have this wonderful doctor, a specialist in growth hormone deficiency at Johns Hopkins, my insurance company saw fit to over-ride his opinions and his test results based on my past pharmaceutical history! Hello??? How could I have a history of taking GH when I’ve never taken it before?
Of course, I found out late on a Friday afternoon. By then it was too late to call my case worker at the drug company, so we’ll see on Monday what to do about an appeal. My local insurance person is also working on an appeal, but the whole thing sounds like just another long ordeal of finding paperwork, calling people, FedExing stuff, too much work when I just wanted to start feeling better by Thanksgiving. I guess that’s not going to happen, at least by the 2004 one.
As it turns out the insurance company rejected the brand of hGH that was prescribed for me. They gave me the ok for a growth hormone was just FDA-approved for adults on 11/4/04. The day this medication was approved for adults was the day after my insurance said that’s what is preferred for me. In the past, this form of hGH was only approved for children with height issues. Am I going to be a ginuea pig again? The new GH company has assigned a rep for me, has submitted info to the pharmacy, waiting for insurance approval, again.
December 2004 ~ I finally started the Growth Hormone last night – it’s like a rebirth for me. I look forward to having my life back in a few months!
January 2005 ~After a lot of phone calls and paperwork, the insurance company finally came through at the very last minute, just as I needed my second month’s supply. Of course, the pharmacy wouldn’t send it unless they were paid for the first month. They had verbal approval from the insurance, but the actual claim was denied. Talk about a cliff hanger!
Later January 2005 ~I’ve been on the growth hormone for 7 weeks now, and see no change in my tiredness and fatigue. A couple weeks ago, I thought there was a bit of improvement. I even exercised a little again, but that was short lived.
I feel like my stomach is getting bigger, and Tom says my face is looking more Cushie again. Maybe from the cortisone I’ve been taking since October. I can’t wait until my next endo appointment in March to increase my GH. I want to feel better already!
March 2005 ~ My IGF-1 was “normal” so I can’t increase the GH.
September 2005 ~ I don’t see any benefit with the growth hormone.
January 2006 ~A new year, a new insurance battle. Once again, they don’t want to pay so I have to go through the whole approval process again. This involves phone calls to Norditropin (the company that makes the GH), my endo, iCore Specialty Pharmacy (the people who prepare and ship the meds) and my insurance company. This is turning into a full-time job!
April 14, 2006 ~I just went to see my endo again on Thursday to see how things are. Although I know how they are – I’m still tired, gaining a little weight, getting some red spots (petechiae) on my midsection. He also noted that I have a “little” buffalo hump again.
My endo appointment is over. Turns out that the argenine test that was done 2 years ago was done incorrectly. The directions were written unclearly and the test run incorrectly, not just for me but for everyone who had this test done there for a couple years. My endo discovered this when he was writing up a research paper and went to the lab to check on something.
So, I’m off GH again for 2 weeks, then I’m supposed to be retested. The “good news” is that the argenine test is only 90 minutes now instead of 3 hours.
April 27, 2006 ~ Wow, what a nightmare my argenine retest started! I went back for that. Although the test was shorter, I got back to my hotel and just slept and slept. I was so glad that I hadn’t decided to go home after the test.
The next day I felt fine and drove back home, no problem. I picked up my husband for a biopsy and took him to an outpatient surgical center. While I was there waiting for the biopsy to be completed, I started noticing blood in my urine and major abdominal cramps. I left messages for several of my doctors on what I should do. I finally decided to see my PCP after I got my husband home.
When Tom was done with his testing, his doctor took one look at me and asked if I wanted an ambulance. I said no, that I thought I could make it to the emergency room ok – Tom couldn’t drive because of the anesthetic they had given him. I barely made it to the ER and left the car with Tom to park. Tom’s doctor followed us to the ER and became my new doctor.
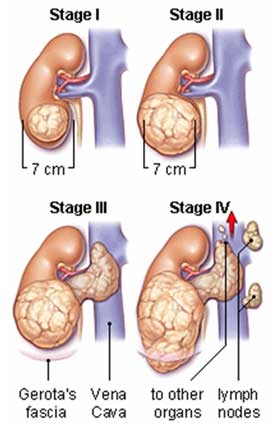
They took me in pretty fast since I was in so much pain, and had the blood in my urine. They thought it was a kidney stone. After a CT scan, my new doctor said that, yes, I had a kidney stone but it wasn’t the worst of my problems, that I had kidney cancer. Wow, what a surprise that was! I was admitted to that hospital, had more CT scans, MRIs, bone scans, they looked everywhere.
My open radical nephrectomy was May 9, 2006, in another hospital from the one where the initial diagnosis was made. My surgeon felt that he needed a specialist from that hospital because he believed preop that my tumor had invaded into the vena cava because of its appearance on the various scans. Luckily, that was not the case.
My entire left kidney and the encapsulated cancer (10 pounds worth!) were removed, along with my left adrenal gland and some lymph nodes. Although the cancer (renal cell carcinoma AKA RCC) was very close to hemorrhaging, the surgeon believes he got it all. He said I was so lucky. If the surgery had been delayed any longer, the outcome would have been much different. I will be repeating the CT scans every 3 months, just to be sure that there is no cancer hiding anywhere. As it turns out, I can never say I’m cured, just NED (no evidence of disease). This thing can recur at any time, anywhere in my body.
I credit the argenine re-test with somehow aggravating my kidneys and revealing this cancer. Before the test, I had no clue that there was any problem. The argenine test showed that my IGF is still low but due to the kidney cancer I cannot take my growth hormone for another 5 years – so the test was useless anyway, except to hasten this newest diagnosis.
August 19, 2006 ~ I’ve been even more tired than usual now that I’m off GH. But I also had cancer.
October 2006 ~ I went to see my Johns Hopkins endo again last week. He doesn’t “think” that my cancer was caused by the growth hormone although it may well have encouraged the tumor to grow faster than it would have.
I was so stupid way back in 1987 when I thought that all my troubles would be over when my pituitary surgery was over.
2016/2017 ~ So. My 10 year kidney cancer anniversary passed, then 11.
May 4, 2017 ~ My endo at Hopkins and I talked about maybe trying growth hormone again. We tested my levels locally and – surprise – everything is low, again.
So, we started the insurance routine again. My insurance rejected the growth hormone I took last time around. I just love how someone, a non-doctor who doesn’t know me, can reject my person endocrinologist’s recommendation. My endo who specializes in Growth Hormone, who runs clinical trials for Johns Hopkins on “Control of growth hormone secretion, genetic causes of growth hormone deficiency, consequences of growth hormone deficiency.”
That insurance person has the power over the highly trained physician. Blows my mind.
But I digress. My doctor has agreed to prescribe Omnitrope, the insurance-guy’s recommendation.
June 14, 2017 ~ I got a call from my insurance. They “may” need more information from my doctor…and they need it in 72 hours.
My doctor’s nurse says that they have to refer this to their pharmacy.
June 15, 2017 ~ I got a call from the Omnitrope folks who said they will need approval from my insurance company <sigh> but they will send me a starter prescription of 30 days worth.
June 16, 2017 ~ I got a call from the Specialty Pharmacy. They’re sending the first month supply on Tuesday. Estimated co-pay is $535 a month. I may have to rethink this whole thing 😦 We sure don’t have an extra $6000.00 a year, no matter how much better it might make me feel.
June 19, 2017 ~ The kit arrived with everything but the actual meds and sharps.
June 20, 2017 ~ The meds and sharps arrived along with the receipt. My insurance paid nearly $600 – and they took my copay out of my credit card for $533.
I still have to wait for the nurse’s visit to use this, even though I’ve used it in the past.
I’ve been doing some serious thinking in the last 24 hours. Even if I could afford $533 a month for this, should I spend this kind of money on something that may, or may not, help, that may, or may not, give me cancer again. We could do a couple cruises a year for this much money. I’ve pretty much decided that I shouldn’t continue, even though I haven’t taken the first dose of this round.
What will happen?
Stay tuned!