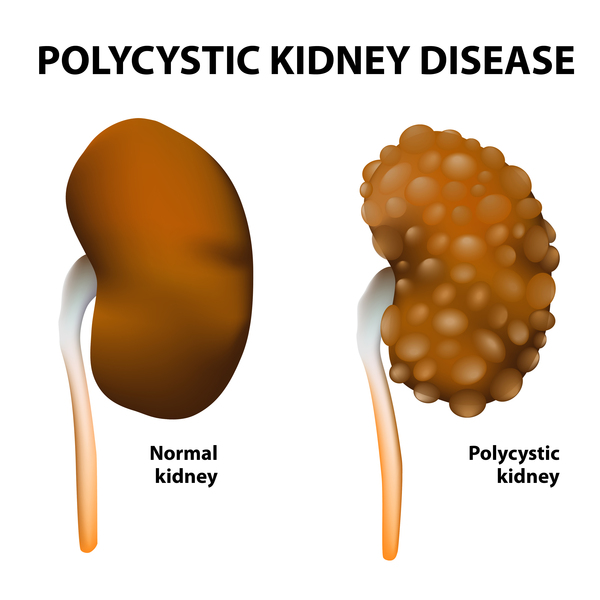
Polycystic kidney disease is a genetic disorder that causes numerous cysts to grow in the kidneys. A kidney cyst is an abnormal sac filled with fluid. PKD cysts can greatly enlarge the kidneys while replacing much of their normal structure, resulting in chronic kidney disease (CKD), which causes reduced kidney function over time. CKD may lead to kidney failure, described as end-stage kidney disease or ESRD when treated with a kidney transplant or blood-filtering treatments called dialysis. The two main types of PKD are autosomal dominant PKD and autosomal recessive PKD.
PKD cysts are different from the usually harmless “simple” cysts that often form in the kidneys later in life. PKD cysts are more numerous and cause complications, such as high blood pressure, cysts in the liver, and problems with blood vessels in the brain and heart.
[Top]
A gene mutation, or defect, causes polycystic kidney disease. Genes provide instructions for making proteins in the body. A gene mutation is a permanent change in the deoxyribonucleic acid (DNA) sequence that makes up a gene. In most cases of PKD, a person inherits the gene mutation, meaning a parent passes it on in his or her genes. In the remaining cases, the gene mutation develops spontaneously. In spontaneous cases, neither parent carries a copy of the mutated gene.
Researchers have found three different gene mutations associated with PKD. Two of the genes are associated with autosomal dominant PKD. The third gene is associated with autosomal recessive PKD. Gene mutations that cause PKD affect proteins that play a role in kidney development.
[Top]
Each cell contains thousands of genes that provide the instructions for making proteins for growth and repair of the body. If a gene has a mutation, the protein made by that gene may not function properly, which sometimes creates a genetic disorder. Not all gene mutations cause a disorder.
People inherit two copies of most genes; one copy from each parent. A genetic disorder occurs when one or both parents pass a mutated gene to a child at conception. A genetic disorder can also occur through a spontaneous gene mutation, meaning neither parent carries a copy of the mutated gene. Once a spontaneous gene mutation has occurred, a person can pass it to his or her children.
Read more about genes and genetic conditions in the U.S. National Library of Medicine’s (NLM’s) Genetics Home Reference External NIH Link.
[Top]
Estimates of PKD’s prevalence range from one in 400 to one in 1,000 people.1 According to the United States Renal Data System, PKD accounts for 2.2 percent of new cases of kidney failure each year in the United States. Annually, eight people per 1 million have kidney failure as a result of PKD.2
Polycystic kidney disease exists around the world and in all races. The disorder occurs equally in women and men, although men are more likely to develop kidney failure from PKD. Women with PKD and high blood pressure who have had more than three pregnancies also have an increased chance of developing kidney failure.
[Top]
Autosomal dominant PKD is the most common form of PKD and the most common inherited disorder of the kidneys.3 The term autosomal dominant means a child can get the disorder by inheriting the gene mutation from only one parent. Each child of a parent with an autosomal dominant mutation has a 50 percent chance of inheriting the mutated gene. About 10 percent of autosomal dominant PKD cases occur spontaneously.4
The following chart shows the chance of inheriting an autosomal dominant gene mutation:

Health care providers identify most cases of autosomal dominant PKD between the ages of 30 and 50.4 For this reason, health care providers often call autosomal dominant PKD “adult PKD.” However, the onset of kidney damage and how quickly the disorder progresses varies. In some cases, cysts may form earlier in life and grow quickly, causing symptoms in childhood.

The cysts grow out of nephrons, the tiny filtering units inside the kidneys. The cysts eventually separate from the nephrons and continue to enlarge. The kidneys enlarge along with the cysts—which can number in the thousands—while roughly retaining their kidney shape. In fully developed autosomal dominant PKD, a cyst-filled kidney can weigh as much as 20 to 30 pounds.
[Top]
In many cases, PKD does not cause signs or symptoms until cysts are half an inch or larger. When present, the most common symptoms are pain in the back and sides—between the ribs and hips—and headaches. The pain can be temporary or persistent, mild or severe. Hematuria—blood in the urine—may also be a sign of autosomal dominant PKD.
[Top]
The complications of autosomal dominant PKD include the following:
- Pain. Cyst infection, other types of urinary tract infections (UTIs), bleeding into cysts, kidney stones, or stretching of the fibrous tissue around the kidney because of cyst growth can cause pain in the area of the kidneys.
- High blood pressure. High blood pressure is present in about half of the people with autosomal dominant PKD and normal kidney function between the ages of 20 and 35.4 Almost 100 percent of people with kidney failure and autosomal dominant PKD have high blood pressure.1 High blood pressure—greater than 140/90 mm Hg—increases the likelihood of heart disease and stroke, as well as adding to the damage already done to the kidneys by the cysts.
- Kidney failure. Kidney failure means the kidneys no longer work well enough to maintain health. A person with kidney failure may have the following symptoms:
- little or no urination
- edema—swelling, usually in the legs, feet, or ankles and less often in the hands or face
- drowsiness
- fatigue, or feeling tired
- generalized itching or numbness
- dry skin
- headaches
- weight loss
- appetite loss
- nausea
- vomiting
- sleep problems
- trouble concentrating
- darkened skin
- muscle cramps
- shortness of breath
- chest pain
Untreated kidney failure can lead to coma and death. More than half of people with autosomal dominant PKD progress to kidney failure by age 70.1
- UTIs. Kidney cysts block the flow of urine through the kidneys. Stagnant urine can set the stage for infection. Bacteria enter the urinary tract through the urethra and spread up to the kidneys. Sometimes, the kidney cysts become infected. UTIs may cause scarring in the kidneys.
- Kidney stones. About 20 percent of people with autosomal dominant PKD have kidney stones.1Kidney stones can block the flow of urine and cause pain.
- Liver cysts. Liver cysts are the most common nonkidney complication of autosomal dominant PKD.1Liver cysts generally cause no symptoms.
- Pancreatic cysts. PKD can also cause cysts in the pancreas. Pancreatic cysts rarely cause pancreatitis—inflammation, or swelling, of the pancreas.
- Abnormal heart valves. Abnormal heart valves may occur in up to 25 percent of people with autosomal dominant PKD.1 Insufficient blood flow in the aorta—the large artery that carries blood from the heart—may result from the abnormal heart valves.
- Diverticula. Diverticula are small pouches, or sacs, that push outward through weak spots in the colon wall. This complication is more common in people with PKD who have kidney failure.1
- Brain aneurysms. An aneurysm is a bulge in the wall of a blood vessel. Aneurysms in the brain might cause headaches that are severe or feel different from other headaches. Brain aneurysms can rupture, or break open, causing bleeding inside the skull. A ruptured aneurysm in the brain is a life-threatening condition and requires immediate medical attention.
[Top]
Health care providers diagnose autosomal dominant PKD using imaging tests and genetic testing.
Imaging Tests
A radiologist—a doctor who specializes in medical imaging—will interpret the images produced by the following imaging tests:
- Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. An abdominal ultrasound can create images of the entire urinary tract or focus specifically on the kidneys. A specially trained technician performs the procedure in a health care provider’s office, an outpatient center, or a hospital. A patient does not need anesthesia. The images can show cysts in the kidneys.

- CT scans use a combination of x-rays and computer technology to create images. For a CT scan, a health care provider may give the patient an injection of a special dye, called contrast medium. CT scans require the patient to lie on a table that slides into a donutshaped device where the x-rays are taken. An x-ray technician performs the procedure in an outpatient center or a hospital. Adults do not need anesthesia. A health care provider may give infants and children a sedative to help them fall asleep for the test. CT scans can show more precise images of cysts in the kidneys.
- Magnetic resonance imaging (MRI) machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x-rays. An MRI may include the injection of contrast medium. With most MRI machines, the patient lies on a table that slides into a tunnel-shaped device that is often open ended or closed at one end; some machines allow the patient to lie in a more open space. A specially trained technician performs the procedure in an outpatient center or a hospital. A patient does not need anesthesia, though a health care provider may use light sedation for people with a fear of confined spaces. A health care provider can use MRIs to measure kidney and cyst volume and monitor kidney and cyst growth, which can help track progression of the disorder.
Kidney imaging findings vary widely, depending on a person’s age. Younger people usually have fewer and smaller cysts. Health care providers have therefore developed specific criteria for diagnosing the disorder with kidney imaging findings, depending on age. For example, the presence of at least two cysts in each kidney by age 30 in a person with a family history of the disorder can confirm the diagnosis of autosomal dominant PKD. A family history of autosomal dominant PKD and cysts found in other organs make the diagnosis more likely.
Genetic Testing
The health care provider may refer a person suspected of having autosomal dominant PKD to a geneticist—a doctor who specializes in genetic disorders. For a genetic test, the geneticist takes a blood or saliva sample and analyzes the DNA for gene mutations that cause autosomal dominant PKD, called PKD1 andPKD2, or autosomal recessive PKD, called PKHD1. Personnel in specialized labs generally perform all genetic testing. A patient may not receive the results for several months because of the complexity of the testing.
Genetic testing can show whether a person’s cells carry a gene mutation that causes autosomal dominant PKD. A health care provider may also use genetic testing results to determine whether someone with a family history of PKD is likely to develop the disorder in the future. Prenatal testing can diagnose autosomal recessive PKD in unborn children.
Two factors limit the usefulness of genetic testing for PKD:
- Detection of a mutated gene cannot predict the onset of symptoms or how serious the disorder will be.
- Even if a health care provider finds a mutated gene, no specific cure for the disorder exists.
[Top]
People who are considering genetic testing may want to consult a genetics counselor. Genetic counseling can help family members understand how test results may affect them individually and as a family. Genetic counseling is provided by genetics professionals—health care professionals with specialized degrees and experience in medical genetics and counseling. Genetics professionals include geneticists, genetics counselors, and genetics nurses.
Genetics professionals work as members of health care teams, providing information and support to individuals or families who have genetic disorders or a higher chance of having an inherited condition. Genetics professionals
- assess the likelihood of a genetic disorder by researching a family’s history, evaluating medical records, and conducting a physical exam of the patient and other family members
- weigh the medical, social, and ethical decisions surrounding genetic testing
- provide support and information to help a person make a decision about testing
- interpret the results of genetic tests and medical data
- provide counseling or refer individuals and families to support services
- serve as patient advocates
- explain possible treatments or preventive measures
- discuss reproductive options
Genetic counseling may be useful when a family member is deciding whether to have genetic testing and again later when test results are available.
[Top]
Although a cure for autosomal dominant PKD is not currently available, treatment can ease symptoms and prolong life. Treatments for the symptoms and complications of autosomal dominant PKD include the following:
- Pain. A health care provider will first determine what is causing the pain and then recommend treatment. If cyst growth is causing persistent pain, the health care provider may first suggest over-the-counter pain medications such as aspirin or acetaminophen. People should consult their health care provider before taking any over-thecounter medication because some may be harmful to the kidneys. For most cases of severe pain due to cyst growth, surgery to shrink cysts can temporarily relieve pain in the back and sides. However, surgery does not slow the disorder’s progression toward kidney failure.
- High blood pressure. Keeping blood pressure under control can slow the effects of autosomal dominant PKD. Lifestyle changes and various medications can lower high blood pressure. Some health care providers recommend blood pressure medications called angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs). Health care providers have found these medications to protect the kidneys in people with other forms of kidney disease besides autosomal dominant PKD. Sometimes a patient can control blood pressure through diet and exercise alone.
- Kidney failure. After many years, PKD can cause the kidneys to fail. Kidneys are essential for life, so people with kidney failure must receive either dialysis or a kidney transplant to replace kidney function. The two forms of dialysis are hemodialysis and peritoneal dialysis. Hemodialysis uses a machine to circulate a patient’s blood through a filter outside the body. Peritoneal dialysis uses the lining of the abdomen to filter the blood inside the body. A kidney transplant is surgery to place a healthy kidney from a person who has just died or a living person, most often a family member, into the patient’s body. People with autosomal dominant PKD have no more complications after transplantation than people with kidney failure from other causes.1
- UTIs. People with autosomal dominant PKD tend to have frequent UTIs, which health care providers treat with antibiotics. People with the disorder should seek treatment for a UTI immediately because infection can spread through the urinary tract to the kidney cysts. Cyst infections are difficult to treat because many antibiotics do not reach the cysts.
- Kidney stones. Treatment of kidney stones in people with autosomal dominant PKD is similar to treatment in people without the disorder. Potassium citrate, taken by mouth, is useful for treating the types of kidney stones associated with autosomal dominant PKD. Breaking up stones with shock waves and removing stones through a small incision do not cause more complications in people with autosomal dominant PKD than in people without the disorder.
- Liver cysts. Most people with liver cysts do not need treatment. A health care provider may aspirate—drain with a needle through the skin—liver cysts in people who have symptoms. In the most severe cases, a patient may need a liver transplant. Infections in liver cysts can be treated with antibiotics and aspiration.
- Pancreatitis. Treatment for pancreatitis usually involves a hospital stay with intravenous (IV) fluids and antibiotics.
- Abnormal heart valves. Abnormal heart valves in people with autosomal dominant PKD rarely require valve replacement. A patient may need further tests if a health care provider detects a heart murmur—a blowing, whooshing, or rasping sound heard with a stethoscope during a heartbeat.
- Diverticula. A high-fiber diet and pain medications help relieve symptoms when diverticula are present. Uncomplicated infection of the diverticula with mild symptoms usually requires the person to rest, take oral antibiotics, and be on a liquid diet for a period of time. Sometimes an infection is serious enough to require a hospital stay, IV antibiotics, and possibly surgery.
- Brain aneurysms. People with autosomal dominant PKD should see a health care provider if they have severe or recurring headaches—even before considering over-the-counter pain medications. Small aneurysms rarely require surgery. A person with a brain aneurysm should avoid smoking and control blood pressure and lipids—fats in the blood.
[Top]
Autosomal recessive PKD is a rare genetic disorder that affects the liver as well as the kidneys. The signs of autosomal recessive PKD frequently appear in the earliest months of life, even in the womb, so health care providers often call it “infantile PKD.” In an autosomal recessive disorder, the child has to inherit the gene mutation from both parents to have an increased likelihood for the disorder. The chance of a child inheriting autosomal recessive mutations from both parents with a gene mutation is 25 percent, or one in four. If only one parent carries the mutated gene, the child will not get the disorder, although the child may inherit the gene mutation. The child is a “carrier” of the disorder and can pass the gene mutation to the next generation. Genetic testing can show whether a parent or child is a carrier of the mutated gene. Autosomal recessive disorders do not typically appear in every generation of an affected family.
The following chart shows the chance of inheriting an autosomal recessive mutation from parents who both carry the mutated gene:

Read more about how people inherit genetic conditions at the NLM’s Genetics Home ReferenceExternal NIH Link.
[Top]
An early sign of autosomal recessive PKD is an enlarged kidney, seen in a fetus or an infant using ultrasound. Kidney function is crucial for early physical development, so children with autosomal recessive PKD and decreased kidney function are usually smaller-than-average size, a condition called growth failure.
Some people with autosomal recessive PKD do not develop signs or symptoms until later in childhood or even adulthood.
[Top]
Babies with the most severe cases of autosomal recessive PKD often die hours or days after birth because they cannot breathe well enough to sustain life. Their lungs do not develop as they should during the prenatal period. Pressure from enlarged kidneys also contributes to breathing problems.
Children born with autosomal recessive PKD often develop kidney failure before reaching adulthood.
Liver scarring occurs in all people with autosomal recessive PKD and is usually present at birth. However, liver problems tend to become more of a concern as people with autosomal recessive PKD grow older. Liver scarring can lead to progressive liver dysfunction and other problems.
Additional complications of autosomal recessive PKD include high blood pressure and UTIs.
[Top]
Health care providers diagnose autosomal recessive PKD with ultrasound imaging, even in a fetus or newborn. The test can show enlarged kidneys with an abnormal appearance. However, a health care provider rarely sees large cysts such as those in autosomal dominant PKD. Ultrasound imaging can also show scarring of the liver.
[Top]
Treatments for the symptoms and complications of autosomal recessive PKD include the following:
- Enlarged kidney. No treatment to prevent or reverse kidney enlargement is available. A patient may need removal of one or both kidneys if pressure from the enlarged kidneys makes breathing impossible. Children with removed kidneys must receive dialysis or a kidney transplant.
- Growth failure. A health care provider should address physical development through nutritional therapy. In severe cases of growth failure in children, a health care provider may consider human growth hormone.
- Breathing problems. Health care providers treat infants with breathing problems with artificial ventilation and, in urgent cases, resuscitative efforts, such as artificial respiration and heart massage.
- Kidney failure. Peritoneal dialysis is the preferred method of treating children with kidney failure, although health care providers also use hemodialysis. Kidney transplantation may be limited in infants because of their size.
- High blood pressure. A health care provider can help control blood pressure with medications.
- UTIs. A health care provider can treat UTIs with antibiotics.
- Liver disease. If serious liver disease develops, some children may need to undergo combined liver and kidney transplantation.
[Top]
Scientists have not yet found a way to prevent PKD. However, people with PKD may slow the progression of kidney damage caused by high blood pressure through lifestyle changes, diet, and blood pressure medications. People with PKD should be physically active 30 minutes a day most days of the week. See “Eating, Diet, and Nutrition” for diet advice on lowering blood pressure and slowing the progression of kidney disease in general. If lifestyle and diet changes do not control a person’s blood pressure, a health care provider may prescribe one or more blood pressure medications, including ACE inhibitors or ARBs.
[Top]
Eating, Diet, and Nutrition
A dietitian specializes in helping people who have kidney disease choose the right foods and plan healthy meals. People with any kind of kidney disease, including PKD, should talk with a dietitian about foods that should be added to their diet and foods that might be harmful.
PKD may require diet changes for blood pressure control. Kidney disease in general also calls for certain diet changes.
Following a healthy eating plan can help lower blood pressure. A health care provider may recommend the Dietary Approaches to Stop Hypertension (DASH) eating plan, which focuses on fruits, vegetables, whole grains, and other foods that are heart healthy and lower in sodium, which often comes from salt. The DASH eating plan
- is low in fat and cholesterol
- features fat-free or low-fat milk and dairy products, fish, poultry, and nuts
- suggests less red meat, sweets, added sugars, and sugar-containing beverages
- is rich in nutrients, protein, and fiber
More information about the DASH eating planExternal NIH Link is available from the National Heart, Lung, and Blood Institute.
As your kidneys become more damaged, you may need to eat foods that are lower in phosphorus and potassium. The health care provider will use lab tests to watch your levels.
Foods high in potassium include
- bananas
- oranges
- potatoes
- tomatoes
Lower-potassium foods include
- apples
- peaches
- carrots
- green beans
Foods higher in phosphorus include
- large portions of meat, fish and dairy foods
- bran cereals and oatmeal
- beans and nuts
- colas
Lower-phosphorus alternatives include
- fresh fruits and vegetables
- breads
- pasta
- rice
- corn and rice cereals
- light-colored sodas
People with kidney disease and high blood pressure should also limit how much sodium they get to 2,300 mg or less each day.5
People with CKD may need to watch how much protein they eat. Everyone needs protein. However, protein breaks down into wastes the kidneys must remove. Large amounts of protein make the kidneys work harder. High-quality proteins such as meat, fish, and eggs create fewer wastes than other sources of protein. Beans, whole grains, soy products, nuts and nut butters, and dairy products can also be good sources of protein. Most people eat more protein than they need. Eating high-quality protein and smaller portions of protein can help protect the kidneys.
More information about nutrition for kidney disease is provided in the NIDDK health topics:
The National Kidney Disease Education Program offers a series of easy-to-read fact sheets about nutrition for people with CKD.
[Top]
- Polycystic kidney disease (PKD) is a genetic disorder that causes numerous cysts to grow in the kidneys.
- A gene mutation, or defect, causes polycystic kidney disease.
- Autosomal dominant PKD is the most common form of PKD and the most common inherited disorder of the kidneys.
- Health care providers identify most cases of autosomal dominant PKD between the ages of 30 and 50.
- The most common symptoms of PKD are pain in the back and sides—between the ribs and hips—and headaches. The pain can be temporary or persistent, mild or severe. Hematuria—blood in the urine—may also be a sign of autosomal dominant PKD.
- The complications of autosomal dominant PKD include the following:
- pain
- high blood pressure
- kidney failure
- urinary tract infections (UTIs)
- kidney stones
- liver cysts
- pancreatic cysts
- abnormal heart valves
- diverticula
- brain aneurysms
- A health care provider diagnoses autosomal dominant PKD using imaging tests and genetic testing.
- A radiologist—a doctor who specializes in medical imaging—will interpret the images produced by the following imaging tests:
- ultrasound
- computerized tomography scans
- magnetic resonance imaging
- Genetic testing can show whether a person’s cells carry a gene mutation that causes autosomal dominant PKD. A health care provider may also use genetic testing results to determine whether someone with a family history of PKD is likely to develop the disorder in the future. Prenatal testing can diagnose autosomal recessive PKD in unborn children.
- Although a cure for autosomal dominant PKD is not currently available, treatment can ease symptoms and prolong life.
- Autosomal recessive PKD is a rare genetic disorder that affects the liver as well as the kidneys.
- The complications of autosomal recessive PKD include the following:
- death due to breathing problems
- kidney failure
- liver scarring
- high blood pressure
- UTIs
- A health care provider diagnoses autosomal recessive PKD with ultrasound imaging, even in a fetus or newborn.
- Treatments for autosomal recessive PKD focus on the symptoms and complications.
- Scientists have not yet found a way to prevent PKD. However, people with PKD may slow the progression of kidney damage caused by high blood pressure through lifestyle changes, diet, and blood pressure medications.
- People with any kind of kidney disease, including PKD, should talk with a dietitian about foods they should add to their diet and foods that might be harmful.
[Top]
1
2
3
4
5
[Top]
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for youExternal NIH Link.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.govExternal Link Disclaimer.
This information may contain content about medications and, when taken as prescribed, the conditions they treat. When prepared, this content included the most current information available. For updates or for questions about any medications, contact the U.S. Food and Drug Administration toll-free at 1-888-INFO-FDA (1-888-463-6332) or visit www.fda.govExternal Link Disclaimer. Consult your health care provider for more information.
[Top]
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Lisa Guay-Woodford, M.D., University of Alabama at Birmingham; Stefan Somlo, M.D., Yale University; Vicente E. Torres, M.D., Ph.D., Mayo Clinic
This information is not copyrighted. The NIDDK encourages people to share this content freely.
From http://www.niddk.nih.gov/health-information/health-topics/kidney-disease/polycystic-kidney-disease-pkd/Pages/facts.aspx


 Whenever I think of Oxycodone, I’m reminded of the night that I was diagnosed with kidney cancer. I’d just been admitted to a room and someone came to visit me. She offered to buy my Oxy from me. I was stunned. Then, she said she was just kidding.
Whenever I think of Oxycodone, I’m reminded of the night that I was diagnosed with kidney cancer. I’d just been admitted to a room and someone came to visit me. She offered to buy my Oxy from me. I was stunned. Then, she said she was just kidding.