From today’s news. I have actually done this when I was feeling unusual after water aerobics.
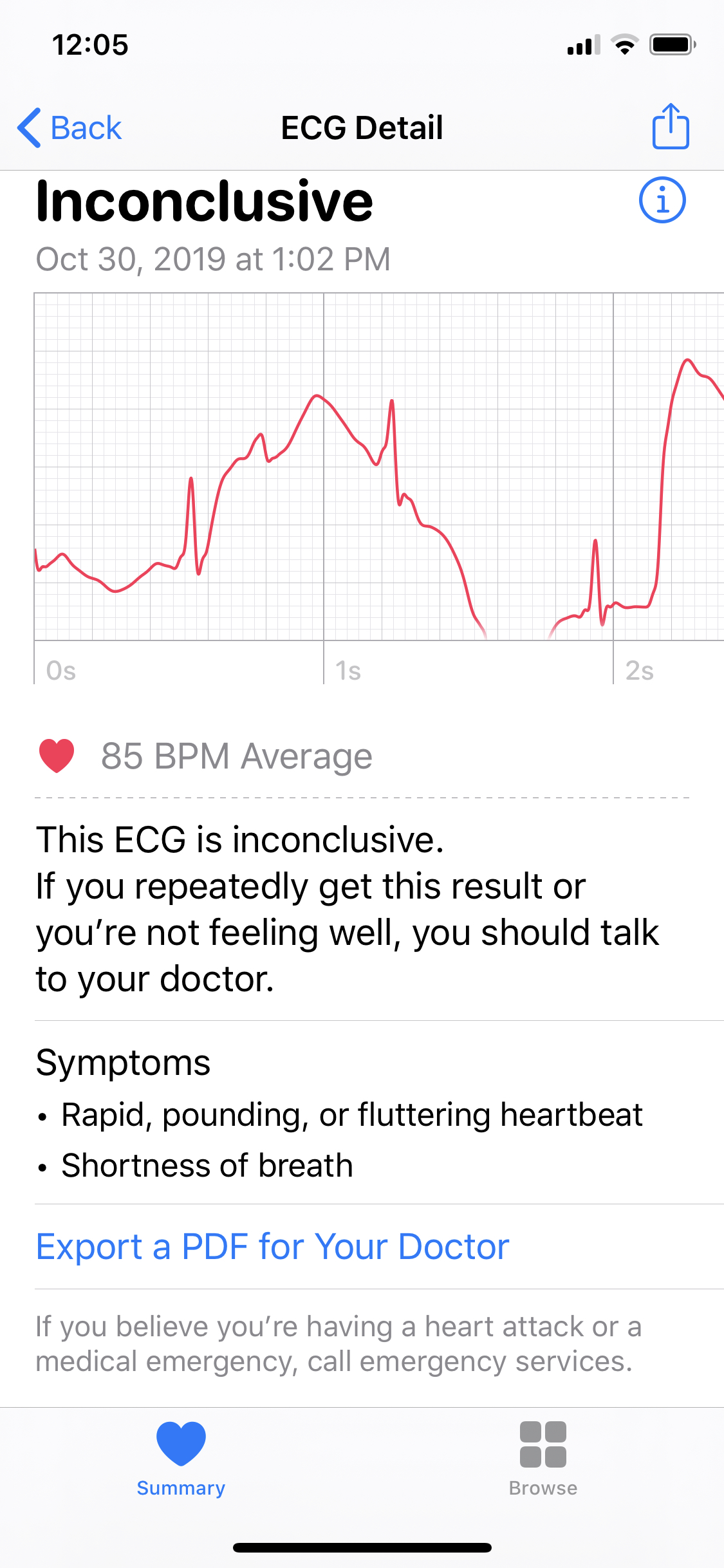
A “quasi-standard” multilead ECG can be recorded using just the Apple Watch, a report showed.
The ECG function on the Watch is designed to monitor electrical activity of the heart in the direction of lead I only, ignoring the superoinferior axis captured by the standard leads (II and III) and the horizontal plane captured by the precordial leads (V1 to V6).
Yet certain workarounds can give the Apple Watch the “quasi-standard” 12-lead information of a proper ECG recording, according to Miguel Ángel Cobos Gil, MD, PhD, of Hospital Clínico San Carlos in Madrid, Spain, reporting online in the Annals of Internal Medicine.
Users can generate lead II by touching the digital crown with a finger on the right hand and lead III by touching with the left hand after moving the smartwatch to the ankle or somewhere on the leg, he said.
And although it’s not possible to generate the conventional precordial leads (V1 to V6), bipolar chest leads (CR1 to CR6) may be sufficient: those can be obtained by placing the back of the watch on the chest and touching the digital crown with a right-hand finger, according to the author.
Cobos Gil showed the similarity in ECG recordings between a standard 12-lead device and the Apple Watch in three test subjects: a healthy person (the author himself), someone with ST-segment-elevation MI, and another with non-ST-segment-elevation MI.
“Standard limb leads (I, II, and III) obtained using both methods are identical, and the precordial leads (V1 to V6 vs. CR1 to CR6) bear a strong resemblance,” he reported.
“Considering the sales figures of Apple devices, the watches likely outnumber conventional ECG machines worldwide. The availability of a method to record an ECG with diagnostic potential anytime and anywhere could potentially revolutionize our approach to cardiac emergencies,” the author suggested.
This report presents a “new twist” on how the Apple Watch can be used and shows that getting the 12-lead information from this device is “definitely something that can be done,” commented Jeffrey Goldberger, MD, of the University of Miami.
But when and why it would be done are unclear, he told MedPage Today in an interview.
Perhaps it could be useful in an urgent scenario where a 12-lead ECG machine is not available, somewhere where medical resources are very limited and there are no hospitals or doctor’s offices around that can do the standard test, he suggested.
Yet the Apple Watch ECG recording would need to be transmitted somewhere to someone who can give advice over the phone — and that would require Internet access. “If it’s a remote area, where do you call for medical care and attention?” Goldberger said.
The smartwatch ECG could be a niche strategy in theory and is certainly not going to replace the conventional machines, he said.
“You need a fair amount of cooperation from the patient to do the various maneuvers to make the various recordings,” he added. “It’s probably more time-consuming to do than just a standard 12-lead where you make the recording and you’re done. Here you do everything in sequence.”
More clinical studies are needed to determine the role of smartwatch ECG recordings, Cobos Gil acknowledged.
Another consumer-oriented device, the AliveCor KardiaMobile 6L, provides 6-lead ECG recordings when paired with a smartphone app.

 Healthy Hearts
Healthy Hearts