Today is the Tenth Anniversary of my kidney cancer surgery. These ten years have been bonus years for me. For my cancer stage, the 5-year survival rate was 81% and I’ve made it twice that long – so far.
What were the odds I’d get kidney cancer? According to my “risk factors”, I “should” have had colon cancer because both parents and an aunt had it twice each. Of course, there’s no guarantee that I won’t get that, too.
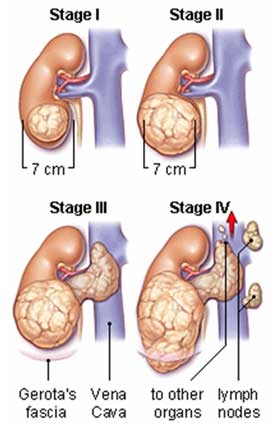
And the risk factors for kidney cancer aka renal cell carcinoma? The majority of kidney cancers are renal cell carcinomas. Risk factors for renal cell carcinoma include:
- Age. Your risk of renal cell carcinoma increases as you age. Renal cell carcinoma occurs most commonly in people 60 and older.
I was younger than this.
- Sex. Men are more likely to develop renal cell carcinoma than women are.
I am female
- Smoking. Smokers have a greater risk of renal cell carcinoma than nonsmokers do. The risk increases the longer you smoke and decreases after you quit.
Not me!
- Obesity. People who are obese have a higher risk of renal cell carcinoma than do people who are considered average weight.
A Cushing’s gift
- High blood pressure (hypertension). High blood pressure increases your risk of renal cell carcinoma, but it isn’t clear why. Some research in animals has linked high blood pressure medications to an increased risk of kidney cancer, but studies in people have had conflicting results.
Never had this until the kidney cancer. It went away immediately post-op but it’s back now.
- Chemicals in your workplace. Workers who are exposed to certain chemicals on the job may have a higher risk of renal cell carcinoma. People who work with chemicals such as asbestos, cadmium and trichloroethylene may have an increased risk of kidney cancer.
What? Me work?
- Treatment for kidney failure. People who receive long-term dialysis to treat chronic kidney failure have a greater risk of developing kidney cancer. People who have a kidney transplant and receive immunosuppressant drugs also are more likely to develop kidney cancer.
Nope. Some sites also list polycystic kidney disease. I don’t have that but half my husband’s family does. Hmmm – wonder if that’s contagious
- Von Hippel-Lindau disease. People with this inherited disorder are likely to develop several kinds of tumors, including, in some cases, renal cell carcinoma.
I’ve wondered about this but, you know, it’s too “rare”.
- Hereditary papillary renal cell carcinoma. Having this inherited condition makes it more likely you’ll develop one or more renal cell carcinomas.
Not that I know of.
I am so thankful for all my doctors but today I am thankful for Dr. Amir Al-Juburi who saved my life by removing my kidney cancer (renal cell carcinoma).
April 28 2006 I picked up my husband for a biopsy and took him to an outpatient surgical center. While I was there waiting for the biopsy to be completed, I started noticing blood in my urine and major abdominal cramps. I left messages for several of my doctors on what I should do. I finally decided to see my PCP after I got my husband home.
When Tom was done with his testing, his doctor took one look at me and asked if I wanted an ambulance. I said no, that I thought I could make it to the emergency room ok – Tom couldn’t drive because of the anesthesia they had given him. I barely made it to the ER and left the car with Tom to park. Tom’s doctor followed us to the ER and became my new doctor.
When I was diagnosed in the ER with kidney cancer, Tom’s doctor said that he could do the surgery but that he would recommend someone even more experienced, Dr. Amir Al-Juburi.
Dr. Amir Al-Juburi has been so kind to me, almost like a kindly grandfather might be, and he got rid of all 10 pounds of my kidney and cancer.
I owe him, the original doctor, and my Cushing’s doctors, my life.
From Alice April 29, 2006
I’m not going to go into every detail at this time. I will fill you in on more details as I receive them from Mary and Tom. I’m sure Mary posted on the boards that she recently went back to Johns Hopkins in Baltimore to be retested because the tests that had been done the past year were incorrect and she was getting the wrong dose of hGh for the past year. In any event, she was tested again on Thursday and then returned home. The above is just a preface to create a time frame of events. It isn’t the reason I’ve come here to ask for prayers for Mary.
This is: Mary mentioned to me last week that she had noticed some blood in her urine. She was going to get it checked. As it were, when she returned from Johns Hopkins, she drove her husband, Tom, to get his regular biopsy for his history of prostate cancer.
[MaryO’Note: Alice got the following paragraph wrong. Fact -The biopsy was at an outpatient surgical center. I drove to the ER and left the car with Tom to park.] While in the emergency room, Mary started having cramps in her stomach and when she went to the rest room, discovered a great deal more blood in her urine. Fortunately, she was at the hospital with her husband when this occurred. The cramps were becoming more severe. The doctors checked her out and they found a tumor in one of her kidneys – the tumor is actually the size of the kidney.
At this point and time, the doctors are recommending removal of the kidney and one of her adrenal glands. One surgeon recommended immediate removal of the kidney. Mary and Tom wanted to first talk with her other doctors and will decide on what surgeon performs the surgery. She never left the hospital where she simply went to take Tom for his test. Instead, she was admitted. She had a great deal of pain last night, but it was helped with pain killers. I will provide hospital details later.
She’s scheduled for an MRI later this morning or early afternoon.
I don’t want to go into much more detail except to say that whatever the condition of the tumor, the prognosis is pretty good.
I know how much all of you love her (as I do), how much she’s done with this site, how hard she’s worked to provide you with so much wonderful information about Cushing’s — plus what a good friend she’s been to so many of you. I also know that those of you who talk to her may want to call her. She needs time to go through all the preliminaries before being inundated with calls.
I will do my best to keep you apprised of Mary’s situation as I receive information. When she gives me the go ahead for giving out the hospital and is ready to take calls, I’ll pass the information along.
Please take a moment to send prayers for {{{{{MaryO}}}}} (she’s “our” MaryO on Power Surge, too) that everything will turn out all right and she will get through this crisis with flying colors.
Dearest
~~~~~~~~~~~~~~~
From Alice April 30, 2006
* Addendum: 9:30 AM – made some corrections to the 5 something AM post.
What a beautiful show of love and support.
I spoke to Mary last night. She had the MRI as scheduled. She spoke with her own doctor and they decided on a surgeon, but it means going to another hospital. She said she’d probably be coming home for a day before going in for the surgery.
I hesitated to mention in my first post that the doctors said they * think the kidney tumor is malignant due to it’s size – 5 cm. I’m sure many of you surmised that, or why would the emergency room doctors recommend immediate surgery. However, as I said earlier, Mary and Tom wanted to consult with her own doctor first. She was told that if, in fact, it is kidney cancer and is detected and treated early and confined to the kidney, the chances for a full recovery are good.
Considering what she’s going through, Mary sounded good. Lord knows, she’s been through so much already. God willing, this may resolve some of the other health issues she’s been experiencing.
Knowing Mary, when she returns home for a day before checking into the other hospital for surgery, if she’s up to it, she’ll post here herself and provide you with additional details.
For now, I’ve told you just about all I know.
Keep up those prayers!
Alice
~~~~~~~~~~~~~~~~~~~~~~~~~~
From Alice April 30, 2006
11 AM Update:
Mary had a brain scan this morning. She was supposed to have a bone scan today as well, but they’re doing it tomorrow instead, so they told her she could GO HOME TODAY (until she checks into the other hospital for the surgery)! She’s thrilled to be going home and I’m sure she’ll be here posting to all of you herself. You know Mary can’t stay away from computers very long. I’d venture a guess that if they looked inside, her arteries and veins would look more like computer cables (ducking).
We love Mary – so keep on praying that everything goes well, that the tests all yield good results and that she’ll be getting better ‘n better until she’s finished with this whole ordeal
(please, God!)
Reminds me of the phrase . . .
Good, better, best
Never let it rest
Til the good is better
And the better, BEST!
Alice
~~~~~~~~~~~~~~~~~~~~~~~~~~
From Alice April 30, 2006
Update – 2:15 PM:
Spoke with Mary. She’s home. She’s resting. The brain scan, chest/lung x-ray, abdominal scan all came out clean. The only test remaining that I know of is the bone scan, but it’s excellent that the above tests yielded good results.
She’s going back to the hospital for the bone scan tomorrow and, hopefully, scheduled for surgery ASAP.
Her attitude is very good. She sounds very good and I know, with God watching over her, and everyone showing so much love and caring, she’ll pull through this with flying colors.
It’s easier for me in conveying information to you to do so with an upbeat attitude. I try to avoid thinking of these things as tragedies or things that make me sick. Of course, I’m saddened and sorry that Mary is going through this — and has gone through so much, but such is life. You all certainly know that very well. Nobody hands us a guarantee that life is going to be without problems. And, yes, as the Morton’s salt container says, It never rains, it pours. But my M.O. is to try to keep as positive as possible, especially when in the throes of life’s unanticipated crises.
I believe the expression, “Attitude” is half the battle won.
Mary’s attitude is excellent and I know in my heart she’s going to come through this just fine.
Alice
P.S. An expression I remember my mother using, “The things we fear never happen. It’s the things we never think about that do!”
~~~~~~~~~~~~~~~~~~~~~~~~~~
From Alice May 2, 2006
There wasn’t much to add yesterday. Mary was scheduled for a bone scan, but first had to have the radioactive tracer substance injection (I presume it was injected — she wasn’t sure herself). She was scheduled to have that around 10:30-11 AM, ET, and then had to return five hours later for the bone scan.
I didn’t speak with her last night, but she text messaged me around 6:30 that she was finally home and that the surgery had been scheduled for a week from today, Tuesday, May 9th at 9:30 AM.
I’ll post the hospital information as the time draws near.
That’s about it for now. She’s still sounding pretty good and wants to get the surgery done already!
Let’s keep those prayers going!
Alice
~~~~~~~~~~~~~~~~~~~~~~
From Me May 2, 2006
First off, I’d like to thank you all for your good wishes, support and prayers. I could do the Sally Field thing and say “…and I can’t deny the fact that you like me, right now, you like me!” but I won’t 🙂
I plan to print everything out and take it with me to the hospital as a cheery-upper.
Alice has been such a wonderful friend through all this, calling, checking up on me, keeping all of you updated on things as they are known right now. Her support and love has been such a wonderful blessing in my life, especially now.
As it is, I’m currently feeling “normal” whatever that is. If I didn’t know I had a problem, I would think that I was just fine.
I am fortunate that I found this out before the tumor could grow any larger. I am fortunate that I was close to the ER, not driving home from Baltimore, or in Baltimore, Oklahoma or on the cruise.
I know that the tumor has been growing for quite a while – it’s very large. I saw the MRI images and even I can tell that it’s not normal. As far as I know now, all the other scans have been fine. I had an abdomen CT, chest CT, brain MRI, chest/abdomen MRI and a full body bone scan.
When I was in the ER Friday, they assumed that it was a kidney stone and did the first abdominal CT scan looking to see where that was. They came back with the news that yes, I had a kidney stone but that it was the least of my worries at the moment. So, I was admitted to the hospital and had all the other scans except the bone scan. Knowing what I know now, it would have been better and easier for me to have had the bone scan as an inpatient. As soon as I checked out and was out of the system, it was harder to get an “emergency” (not scheduled weeks in advance) bone scan. Oh, well.
My surgery will be next Tuesday, May 9, at 9:30AM at Fairfax Hospital (
http://www.inova.org/inovapublic.srt/ifh/index.jsp ). I’m expected to stay there for 3-5 days post op and they don’t anticipate any pesky complications like chemo or radiation at this time.
For now, I’m keeping my normal schedule, avoiding reading horror stories online, eating, sleeping – even napping! – as usual. Sometimes I even forget that I have this little medical appointment next week.
For a non-phone person I’ve talked with so many people these last few days, it’s mind-boggling.
I’m happy to report that all is not lost on the (Cushie) cruise. Someone will replace me – and there will be another cruise later in the year. YEA! My main “concern” on that now is that I’ll lose weight (finally!) post-op and my cruisewear will no longer fit. Yeah, right.
In thinking back, I think it’s a good thing that my arginine test was messed up in Sept of 05. If it hadn’t been, I wouldn’t have redone it on Thursday. I believe that having that stuff in my body was what made my kidneys rebel and act up on Friday. So, without the lab screw-up I might not have known anything for a long time.
So, it’s all good
Thanks to everyone who has called and posted such wonderful things. I cannot begin to imagine what my email looks like…
~~~~~~~~~~~~~~~~~~~~
From Alice May 9, 2006, 09:10 AM
I’ve been in constant contact with Mary. Spoke to her at 7 this morning. She, Tom and their son, Michael, were on the way to the hospital. Mary sounded very good as she has all week. She’s going in with an excellent attitude.
She’s probably being prepped right now. The surgery is set for for 9:30 (ET). They anticipate the surgery will last 3 1/2 – 4 hours.
Now, all we can do is pray and wait. Tom will call me after the surgery is over. As soon as I hear something, I’ll make it a point to come back and post what I know.
Your support, love and prayers have been remarkable. Thank you on behalf of Mary. Please keep on praying until it’s over.
God? You listening? You’ve got someone very special to watch over this morning. We’re counting on you!
Alice
~~~~~~~~~~~~~~~~~~~
From Alice May 9, 2006, 12:33 PM
Mary’s husband, Tom, called me at 12:15
He said it’s going to be another 3 hours – around 3:15 PM – before they’re done. Surgery didn’t start as scheduled at 9:30, but more like 11:30. There wasn’t that much he could tell me except that the doctors said, so far everything is going as expected and Tom said, “so far, so good.”
I hesitate to draw any conclusions from that statement because I’m not 100% sure of what the doctors expected, so it’s a matter of waiting until it’s over.
I’ll keep you posted. Keep praying, please!
Alice
~~~~~~~~~~~~~~~~~~
From Alice May 9, 2006, 2:00PM
Tom called at 1:15, but we had a bad connection. We finally connected.
The operation is over. Mary was being sewn up. Tom said according to the doctor, “the tumor and the kidney were removed.” The doctor is calling the operation a “complete success.”
I asked if they saw any signs of cancer anywhere else because Mary had told me originally that they’d said they might remove the gallbladder, too, but they didn’t remove the gallbladder – which is a good sign.
It appears as though everything was concentrated in the kidney.
Thank God. It’s over!
Alice
~~~~~~~~~~~~~~~~~~~~~~~~
From Alice May 9 2006, 07:39 PM
Someone said: “… I told her that I would wait until she was home and feeling much better before I talked to her again and she agreed that she wasn’t sure she would be up to taking phone calls. Again, thank you so much for keeping us updated… this way we can know how Mary is doing without her having to take so many calls…”
That’s exactly how Tom and I feel. Tom suggests people not call the hospital. I wouldn’t even call his cell phone all day. I waited for him to contact me. I know he’s also exhausted. I figured he’d call when he was up to it. He called about 15 minutes ago.
It’s important that Mary get all the rest she can while recovering. Yes, everything turned out well, but she still had major surgery, is on morphine and needs her sleep. It’s important that we all allow her this time to rest.
It just so happened she was awake when he called and he turned on his cell phone’s speakerphone so Mary and I could talk for a minute. I was so happy to hear her voice. She sounded tired, her mouth was dry, but she sounded good.
Because this is a public message board, I prefer not to post details of the room she’s in. If anyone wants this information for the purpose of sending something to Mary, please E.mail me from the address you registered with on the board, and please include your user name. Thanks.
Another thing is that Mary has allergies, so for those wishing to send something to her, Tom and I (and Mary, as we discussed before she went into the hospital) agree she’s better off without flowers.
Finally, Tom said the doctor was very pleased with how her surgery went – that her body was quite robust, that there was very little bleeding, so no transfusion was needed, and he was generally very pleased with the surgery.
It’s been a very stressful day. I love Mary like a sister. We’ve been good friends for 11 years. I cried so after he initially called and said everything went well. I know all of you love and care about Mary, too.
All I’ve thought all day is, thank you, God, for watching over MaryO. I know all of you have thought the same thing.
That’s about it for now — she even cracked a personal joke when we said goodbye — she’ll be back to her old self again before too long.
Alice
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
From Alice May 13 2006, 08:10 PM
Saturday Update on Mary:
When she’s back on her computer, I know Mary will be thrilled to read all your thoughtful, beautiful and caring messages.
She’s doing well. The worst part is the incision which is quite large because the doctors originally anticipated the possibility of having to remove the adrenal gland above the kidney that was removed and the gall bladder as well. However, as I posted earlier, once they got in there, everything was found to be clean so they just took out the tumor and the kidney (as if that’s not enough). So, when she gets up to go to the bathroom, the incision is quite painful. I imagine an incision of that size will take a while to heal. Other than that she says she feels good!!
Additionally, the doctor was awaiting the results of the lymph node biopsy (just to be sure) and he told her yesterday, “everything looks clean.”
She was originally scheduled to go home tomorrow, Sunday, but . . . she went home TODAY!
Spoke to her after she arrived home (sorry I didn’t post earlier, but also have my Web site to deal with).
She sounded great and was glad to be home especially since a new person checked into her room yesterday and Mary wasn’t able to sleep all night.
That’s all for now – and all very good news, thank God!
Alice
~~~~~~~~~~~~~~~~~~~~~~~~~
From Me: June 17, 2006 post-op:
Thank you all for your prayers, good wishes, cards, phone calls, gifts, general “cheery-uppers”. They all really helped me on my road to recovery.
I do have a ton of thank you cards to send out to lots of people – I’m very slow at that. Under normal circumstances my handwriting is terrible. Now, post-op kidney cancer, I can no longer take my arthritis meds or any NSAIDs and my writing will probably be even worse 😦
I am very nearly better, not much pain anymore, a nasty big scar and my energy levels aren’t so great. Of course, they were awful before. I can no longer take the GH even though I’m deficient. In 5 years (if I survive!) I can take the GH again, supposedly.
I’ve had a lot of time to do a lot of thinking over the last 6 weeks. I know I was extraordinarily lucky to have my tumor discovered before it was too late. The lab reports and my surgeon reported that it would only have been a week or so before the tumor had hemorrhaged and caused major problems. Thank goodness the arginine retest for GH had caused me to bleed – at least I think that’s what set it off. If I hadn’t had all the blood and pain for one day only, I’d have had no clue that I had this cancer and who knows what would have happened in that next week.
I will be getting CT scans every 3 months for awhile to be sure that there is no cancer hiding out.
During my time of thinking, I have also been thinking about making changes to the boards based on what I have heard was going on here. I am not yet sure how these changes will manifest themselves but I do know that bashing others will not be tolerated. More on this later, in another area.
Again, thank you for all your support!
~~~~~~~~~~~~~~~~~~~
From Me July 6, 2006
Since I recently had surgery for kidney cancer, I’ve been looking around for another board to read and talk about this with other survivors (hopefully!) I haven’t found anyplace I’d like to visit or feel comfortable with yet, so I decided to make a new area here.
I know – or I think I know – that no one else here has had kidney cancer, although I know at least 1 other person has had a kidney removed and several others have reported kidney stones and other possible kidney diseases.
I’m sure that my recovery will be much the same as for any other major abdominal surgery, although I’d like it to be faster.
Before my surgery, I didn’t have time really to consider that I had cancer, and what it meant for my life. There was no going from doctor to doctor, running a different test each week, suspecting that maybe… Just boom, there it is. Cancer.
Now that I’m about 8 weeks post-op, I’m thinking more and more about this and how it might affect my future. I know that there are going to be lots of scans, every 3 months, just to be sure that there wasn’t a cell hiding out.
I know I have to be careful with meds – no NSAIDs so my arthritis is worse. No GH – it’s contraindicated for 5 years…assuming I’m cancer free then.
I’m supposed to be eating less protein, more fruits/veggies, drinking more water.
And I’m supposed to avoid playing football and other things that might damage my remaining kidney.
Normally, I know how very lucky I am. I just reread the path reports and know that the tumor was already hemorrhaging around the borders and the cysts contained hemorrhagic fluid. Things could be much worse.
Sometimes, at night when I can’t sleep, I wonder why I was lucky like this. What haven’t I done with my life that I should. Seems to me that I’ve accomplished what I should already.
And, in the night, I worry about the cancer returning, taking my other kidney or worse.
At this time, there’s no standard chemo unless it’s metastasized, although there are some promising clinical trials and radiation doesn’t seem to work for this kind of cancer, so if it returns it’s more surgery.
I suppose I could/should have put all this in my blog, but I put it out here in case anyone else should need this in the future. I hope not!
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
From me Aug 19 2006, 01:25 AM
Thanks so much for asking!
Unfortunately, I haven’t read the boards much lately – I’m spending most of my online time deleting/banning the InstaChat intruders.
I have been working on the websites, though, and that’s always fun! I’ve even added a new one to the roster and it has some cool stuff on it. New features to be announced in the upcoming newsletter.
I’ve been even more tired than usual now that I’m off GH. I can’t take my arthritis meds, or anything like Excedrin (no NSAIDs) so my joints are nearly always bothering me and I have to wait out any headaches. I’m also just getting over a UTI.
I just had my 3 month post-op CT scans and I hope they come out ok. At first I was grateful that I wouldn’t have to have chemo or radiation come to find out that neither has been discovered yet which works well with kidney cancer. Apparently, it can resurface any time for the rest of my life. I’m hoping that some of the chemo clinical trials show some good results so I can get this thing before it metastasizes somewhere.
I’m having trouble sleeping (1:20 AM here, now) although I’m always tired. My mind plays all kinds of tricks in the night. Those InstaChat people don’t help, either! When I wake up just a little, instead of falling back asleep, I’ll go check to see what they’ve done.
Whine, whine!
On the plus side – I survived the kidney cancer surgery, and it’s almost vacation time!
Even vacation will be bittersweet, though. 2 years ago,
Sue went with us on vacation. She had a great time and she had asked if she could go with us again this year. Of course, we had said yes…
~~~~~~~~~~~~~~~~~~~~~~~
From me May 8 2008, 11:07 PM
I am feeling very maudlin, a bit down and depressed. It’s very nearly the anniversary of my kidney cancer surgery. I posted this in my blog a few days ago:
I’ve been feeling weird for about a week now. Last Friday, I went through the whole “Sending Prayers” topic (MKO’Note: this thread) that my good friend Alice started for me.After I read that, I started reliving all the kidney cancer events…again. I know I shouldn’t do this. My counselor says that this is a very stressful thing to do and it’s not good for me, for anyone. But I do it anyway, especially the pituitary and cancer surgery anniversaries. I wish I did this with good stuff, could relive that instead of the scary and painful.
After I finished rereading all that, I went back to my post in the cancer section: I guess I’ve talked about this more than I think! I just wish there was someone I could get answers and support from. I have never met anyone in real life who has shared my particular brand of cancer, haven’t talked to anyone on the phone or emailed anyone.
I even asked at my local cancer support center about support for me – they have all kinds of meetings, mainly for breast and prostate cancer, but other kinds, too. But they said that there weren’t enough kidney cancer people to have a meeting. The one and only book that the library there has on kidney cancer was given to me by the author to donate there.
Lucky me – two rare diseases that no one gets. According to statistics I should be a black man who smokes and works in the iron and steel industry or is exposed to certain chemical and substances, such as asbestos (a mineral fiber that can be used in construction materials for insulation and as fire-retardant) and cadmium (a rare, soft, bluish-white chemical element used in batteries and plastic industry), also increase the risk for renal cell carcinoma. I should have polycystic kidneys and not drink the copious coffee.
So…where did it come from? A mutation of my parents’ and aunt’s colon cancer or do I still have that looming on my horizon?
And the Cushing’s came from nowhere, too. I know that no one knows these answers but I think of them a lot, especially at night.
Although I’m not afraid of death and would like it to be as peaceful and pain-free as possible, I still dream at night that I’m dying or have died. These dreams have been going on since before the cancer and I can’t seem to shake them although I’m taking them more in stride now and can go right back to sleep.
And from last year’s post on this topic, these still concern me:
What if the lung nodules that “aren’t growing” turn out to be something on the next scan? Is the stomach distress I’m currently feeling a cause to ask for my next colonoscopy a bit earlier?
Is the pain on the other side the other kidney causing trouble? Or something new with an ovary?
What if, what if…?
Seems like in my addled brain any new symptom could be cancer, not the simple stomach bug or pulled muscle.
Had they told me in 2006 that I only had a year or two to live, I’d have thought it far too short a time. I guess how long a year is depends on the frame of mind!
I hate going for scans because they could show something but I get nervous when there are no scans because there could be something else! Seems like my mind is setting me up for a lose-lose situation.
I’m sure as I get closer to Friday that other thoughts will come to me. I am so grateful that I’ve had these two “bonus years”. I feel like there is so much still to do with the Cushing’s sites and I will never get them done in my lifetime but I plan to keep trucking along!

And from Wonderful Words of Life…
I’m acquiring the title of an old hymn for this next post.
After I was finished with the long Cushing’s diagnostic process, surgery and several post-op visits to NIH, I was asked to give the scripture reading at my church. The man who did the sermon that week was the survivor of a horrific accident where he and his family were hit by a van while waiting at an airport.
i thought I had written down the verse carefully. I practiced and practiced, I don’t like speaking in front of a crowd but I said I would. When I got to church, the verse was different. Maybe I wrote it down wrong, maybe someone changed it. Whatever.
This verse has come to have so much meaning in my life. When I saw at a book called A Musician’s Book of Psalms each day had a different psalm. On my birthday, there was “my” psalm so I had to buy this book!
Psalm 116 (New International Version)
1 I love the LORD, for he heard my voice;
he heard my cry for mercy.
2 Because he turned his ear to me,
I will call on him as long as I live.
3 The cords of death entangled me,
the anguish of the grave came upon me;
I was overcome by trouble and sorrow.
4 Then I called on the name of the LORD:
“O LORD, save me!”
5 The LORD is gracious and righteous;
our God is full of compassion.
6 The LORD protects the simplehearted;
when I was in great need, he saved me.
7 Be at rest once more, O my soul,
for the LORD has been good to you.
8 For you, O LORD, have delivered my soul from death,
my eyes from tears,
my feet from stumbling,
9 that I may walk before the LORD
in the land of the living.
10 I believed; therefore I said,
“I am greatly afflicted.”
11 And in my dismay I said,
“All men are liars.”
12 How can I repay the LORD
for all his goodness to me?
13 I will lift up the cup of salvation
and call on the name of the LORD.
14 I will fulfill my vows to the LORD
in the presence of all his people.
15 Precious in the sight of the LORD
is the death of his saints.
16 O LORD, truly I am your servant;
I am your servant, the son of your maidservant;
you have freed me from my chains.
17 I will sacrifice a thank offering to you
and call on the name of the LORD.
18 I will fulfill my vows to the LORD
in the presence of all his people,
19 in the courts of the house of the LORD—
in your midst, O Jerusalem.
Praise the LORD.
I carry a print out of this everywhere I go because I find it very soothing. “when I was in great need, he saved me.” This print out is in a plastic page saver. On the other side there is an article I found after my kidney cancer. I first read this in Chicken Soup for the Surviving Soul and is posted several places online.
The Best Day Of My Life
by Gregory M Lousignont
Today, when I awoke, I suddenly realized that this is the best day of my life, ever! There were times when I wondered if I would make it to today; but I did! And because I did I’m going to celebrate!
Today, I’m going to celebrate what an unbelievable life I have had so far: the accomplishments, the many blessings, and, yes, even the hardships because they have served to make me stronger.
I will go through this day with my head held high, and a happy heart. I will marvel at God’s seemingly simple gifts: the morning dew, the sun, the clouds, the trees, the flowers, the birds. Today, none of these miraculous creations will escape my notice.
Today, I will share my excitement for life with other people. I’ll make someone smile. I’ll go out of my way to perform an unexpected act of kindness for someone I don’t even know.
Today, I’ll give a sincere compliment to someone who seems down. I’ll tell a child how special he is, and I’ll tell someone I love just how deeply I care for her and how much she means to me.
Today is the day I quit worrying about what I don’t have and start being grateful for all the wonderful things God has already given me.
I’ll remember that to worry is just a waste of time because my faith in God and his Divine Plan ensures everything will be just fine.
And tonight, before I go to bed, I’ll go outside and raise my eyes to the heavens. I will stand in awe at the beauty of the stars and the moon, and I will praise God for these magnificent treasures.
As the day ends and I lay my head down on my pillow, I will thank the Almighty for the best day of my life. And I will sleep the sleep of a contented child, excited with expectation because know tomorrow is going to be the best day of my life, ever!
When I’m feeling down, depressed or low, reading my 2 special pages can help me more than anything else.